East Toronto Health Partners (ETHP) submit Full Application to become an Ontario Health Team for East Toronto
October 9, 2019
Hon. Christine Elliott
Ontario Deputy Premier and Minister of Health
Hon. Merrilee Fullerton
Ontario Minister of Long-Term Care
College Park, 5th Fl.,
777 Bay St, Toronto
ON M7A 2J3
RE: Ontario Health Team Submission from the East Toronto Health Partners
Dear Ministers Elliott and Fullerton;
In partnership with those who receive care and those who provide care in East Toronto, the East Toronto Health Partners (ETHP) are pleased to submit our full application to become one of Ontario’s first Health Teams. In your call for applications, you invited us to be bold in our thinking, and we have taken this to heart. We also recognize that with the changes envisioned
for health care in Ontario, there are both opportunities and inherent risks. We want you to know that we are fully committed to building a bolder, brighter future for the delivery of health and social care for our local communities, and we look forward to the support of your Ministry to help us transform our systems of care.
Our vision is to work with our community to co-design ‘A System without Discharges’: A seamless continuum of care focused on population health, with programs tailored to our 21 local neighbourhoods and communities. We have grounded our vision in the Quadruple Aim, with goals to improve quality of care and the experience of our patients and caregivers, enhance health and wellness for clinicians and other front-line providers, improve overall population health, and increase the value of investments in health and social care.
About Our Population
Collectively, we serve the approximately 300,000 children, adults and seniors who live in the multiple communities that comprise East Toronto. Our boundaries span from the Don River to the West, to Warden in the East, and from South of Eglinton Ave to Lake Ontario; and include priority neighbourhoods such as Thorncliffe Park and Flemingdon Park. We also serve Ontarians across the Greater Toronto Area and beyond for a total attributed population of 375,000. When our Ontario Health Team reaches maturity, we will have a full population health and integrated care model that supports our entire population; however, in Year 1 we will focus on integrating care for the following three populations:
1. Seniors with chronic care needs and caregivers: East Toronto has a significant population of seniors (53,712) and heavy burden of chronic illnesses including Chronic Obstructive Pulmonary Disease (3,937 people) and Congestive Heart Failure (2,734 people). Seniors with chronic care needs experience high levels of hospital admissions, and long lengths of stay, contributing to hallway medicine pressures. We selected this population because of the risk factors within the East Toronto seniors’ population with chronic care needs, including high rates of caregiver distress (up to 47% in some of our communities). The redesign of care for this population will build on what we’ve heard from patients, families, caregivers, and health care providers about the current challenges they face with fragmented services and poor transitions of care.
2. Youth Mental Health and Wellness: As rates for mental health issues in youth are rising across Toronto and Ontario, some neighbourhoods in our region such as Taylor Massey have three times higher Emergency Department (ED) use for youth mental health than the Toronto average. East Toronto has approximately 7,977 youth living with mental health conditions. Our initial work with youth in East Toronto has identified several opportunities for us to co-design improved access to care and better support youth mental health and well-being.
3. Substance Use and Health: East Toronto providers serve significant numbers of people with issues of substance use. The Canadian Institute for Health Information identified 7,288 people in our attributed population with diagnosed Drug/Alcohol Dependency; often these individuals are disconnected from basic primary care, have significant issues related to the social determinants of health, and have high rates of emergency room use and hospital admission. We have identified opportunities with patients and providers to coordinate harm reduction, treatment, and crisis supports to improve health for this population.
Our work with our priority populations will be grounded in a neighbourhood approach; starting with the five “Neighbourhood Improvement Areas” as defined by the City of Toronto. This neighbourhood-based approach is intended to help us address some of the priority equity considerations facing our population; a high proportion of newcomers and immigrants, patients who are uninsured, individuals and families with lower incomes, and engagement of Indigenous and Francophone populations. Of our total attributed population of 375,000, the 178 family practice physicians who have joined the new East Toronto Family Practice Network (EasT-FPN) care for approximately 200,000 patients. In addition, the priority populations for Year 1 aggregate to roughly 69,000 people.
Through our members and the scope of services we provide, ETHP will provide actively coordinated care for roughly 20% of the total Year 1 population: a total of 13,800 individuals. In addition, the 200,000 residents who access primary care through family physicians who are part of EasT-FPN will have access to integrated care through our SCOPE program, interprofessional care teams, fall/winter community surge investments and other existing programs in East Toronto.
About Our Team and How We Will Work Together
The ETHP are building on a 25-year history of collaboration to improve the health of our local population through collaborations such as Partners for Health and the Solutions Network. In late 2017, the CEOs of five organizations that represent the continuum of healthcare came together to form the foundation for an integrated care network (ETHP). Over the past two years, the ETHP has been working with patients, families, community representatives and a range of partner organizations towards this goal.
In October 2019, the ETHP welcomed our newest Anchor Partner, the East Toronto Family Practice Network (EasT-FPN) which was created to be the representative voice of the over 260 family physicians in East Toronto. EasT-FPN has established an Interim Board of Directors, Interim Executive and a Memorandum of Understanding for engaging with family physicians. Over the next few weeks, EasT-FPN is hosting a series of engagement sessions for family physicians to learn about the work of the ETHP and encourage physicians to participate in the design and development of our Ontario Health Team. To date, 178 family physicians have joined the EasT-FPN, who care for approximately 200,000 patients as part of the ETHP.
The ETHP is governed through an Anchor Partner model, with each member of our anchor organizations representing a different care sector. Our starting point for governance has been a ‘network of networks’ model which has enabled a small group of trusted partners, which represent the full continuum of care, to facilitate change and improve care through a streamlined decision-making process. The current members of the East Toronto Health Partners are:
- Patients, Families and Caregivers** East Toronto Family Practice Network – EasT-FPN
- Michael Garron Hospital (Toronto East Health Network)
- Providence Healthcare (Unity Health Toronto)
- South Riverdale Community Health Centre (on behalf of East Toronto CHCs)
- VHA Home HealthCare (liaison to home care providers)
- WoodGreen Community Services (representing home and community care, community mental health, addictions and developmental services, community support services and housing)
The organizational members above will be formal signatories to the Joint Venture agreement and to the eventual accountability agreement with the Ministry of Health. Our Joint Venture agreement, which will be signed by the Anchor Partners in October 2019, outlines our shared principles, how we will work together, and how our partnership will evolve over time.
In addition, the ETHP network of providers includes two other levels of partnership:
- Engaged Partners, actively involved in the planning and delivery of specific initiatives; and,
- Supporting Partners, who remain informed and involved, but may not be active in planning or delivery.
A letter of support from our partners is included in the supplemental information of our application. Together, all of our partners deliver the full range of services needed to support our Year 1 populations.
**Over the last 6 months, the ETHP has hosted a number of community engagement sessions to involve patients, caregivers and providers in helping us co-design the future of care for our priority populations. To help guide our ongoing work, a Patient and Caregiver Engagement Planning Team consisting of advisors from existing Patient and Family Advisory Committees from several East Toronto organizations was established to advise on different approaches to patient, family, caregiver and community engagement for the ETHP. Our Patient and Caregiver Engagement Planning Team is assisting us with next steps in this work, including a process to identify ongoing membership at the Governance level to ensure patient and caregiver involvement in strategy, priority setting and decision making.
We will continue to work with all our communities as we redesign the future of care in East Toronto. To support this work, the ETHP has developed a Community Engagement Framework; a best practice guideline for current and future engagement activities within the OHT planning context. Patients, community members and providers were engaged in a joint working group with representation from the East and Downtown East OHTs to develop this framework.
How We Will Transform Care
The ETHP see significant opportunities to improve care for our population and health system performance as we create an integrated health system. Our shared vision is centred on creating ‘a system without discharges’; one connected system of health care and support for all residents in East Toronto. Our most important improvement opportunities are fully aligned to this shared vision:
1) Create a one-team approach with patients, caregivers and providers: This includes engaging with care recipients to design care transformations that meet their needs, supporting all our staff to work to their full scope, and building stronger networks between providers who deliver similar and complementary services. For our Year 1 focus, we will expand our existing integrated, interprofessional team-based care models and simplify access to community support services. For our youth and adults with mental health needs, our focus will be on building skills, relationships and trust, to support them with their goals.
2) Coordinated Care tailored to Local Neighbourhoods; scaling up our early successes: This includes evaluating and expanding our existing integrated care initiatives and shifting more care from hospital to community. We will co-design tailored solutions for our 21 neighbourhoods to address their distinctive needs, ranging from designated improvement areas to higher income communities. For our Year 1 focus, we are targeting improvements to three Neighbourhood Improvement Areas; Thorncliffe Park, Taylor-Massey and Oakridge. We will also expand our Home 2Day program to support a broader range of patients with cardiac and respiratory conditions, increase our community investments during the flu season, and expand our interprofessional care team models to other neighbourhoods in partnership with our primary care partners.
3) Support the Success of our New Primary Care Network – The ETHP is very excited to welcome our newest Anchor Partner, the East Toronto Family Practice Network (EasT-FPN). Full engagement of primary care at every level of the ETHP is critical to the success of an integrated model of care in East Toronto. Together, the ETHP will develop multiple ways to engage and connect with local family physicians so they can continue to be an integral part of the design and evolution of integrated care. The ETHP are also working on a financial plan as part of our shared commitment to develop and sustain our partnership.
4) Streamline Access and Navigation, enabled by Digital and Virtual Care: This includes providing easier access to information and access to services, reducing the burden of chronic disease, and improving coordination of care to support patients and their caregivers. For our Year 1 focus, we will: finalize our asset maps of services that support our Year 1 populations; create digital navigation tools for local services such as Youth mental health and wellness programs; and, establish patient navigators to support seniors with chronic disease and caregivers with health system navigation, service planning, care plan accountability, and one touchpoint for hospital to community transitions. For individuals who access the Emergency Department related to substance use we will coordinate access to community services based on similar models implemented at peer hospitals.
5) Improve population health and health equity: This includes reducing gaps in care and improving coordination of services for vulnerable, marginalized and under-served populations. For our Year 1 focus, we are targeting improvements for seniors living in Toronto Community Housing buildings, youth with mental health concerns, and adults with substance use issues.
Our overall vision for care redesign is centred on creating integrated, community-based health and social care teams across our 21 neighbourhoods that will support 24/7 access, and link to acute care, specialty care and other regional services as depicted in the graphic below.
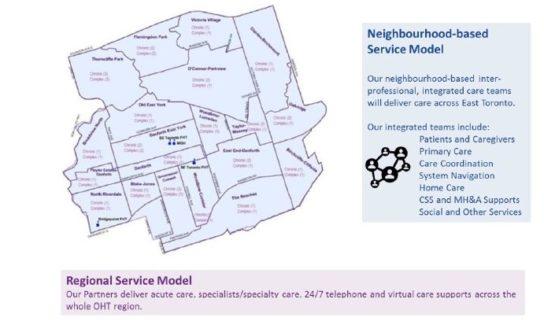
Unlike our current siloed health care system, through our neighbourhood-based model of integrated care, people will experience one local system that provides simple access to health services and social supports, navigation and care coordination, inter-professional/ interorganizational teams, and streamlined communication of health and social care providers. This model focuses on simplifying the system for patients and frontline staff, maximizing current system investments and enhancing efficiency and effectiveness. Key enablers of this model of care are:
- A simplified model for care transitions, with established care pathways that support patients to move easily from hospital to home;
- Integrated, neighbourhood-based care teams, that align interprofessional teams from home care and community support services with primary care;
- Care Coordinator/Navigators aligned to neighbourhoods / specific geographies using existing staffing resources from organizations that currently provide these services;
- Access to regional supports including, but not limited to; acute care, specialty care, 24/7 call centre support services for patients and caregivers, virtual care and remote monitoring; and,
- Digital communications and integrated information systems to support care teams, patients and caregivers with real-time access to patient health information and care plans that address the full social determinants of health.
Digital Health
The ETHP Digital Health Team has created a vision and a strategy for advancing virtual care, access to health information, information sharing, and quality improvement. Our overarching goals for the ETHP Digital Strategy are:
1. Achieving Digital Connectivity – to allow for the exchange of information and open communication that is fundamental to an integrated system of care
2.Digital-First Customer Service – to prioritize solutions that support health equity, positive experiences and flexible virtual care options
3. Fostering an Intelligent Learning System – to optimize our use of population health and care data, advance predictive capabilities, provide centralized supports and enable innovation
Specific solutions included in our Digital Strategy include expanding the use of the MyChart application across our partners, testing a patient-oriented portal, leveraging existing app-based technology to facilitate 24/7 access to support for patients and caregivers, expanding use of virtual visits, and enabling secure messaging between providers (and eventually patients and caregivers). The ETHP are in the process of developing a data-sharing agreement as well as common policies for privacy, security, cyber-security and data governance.
_________________
The Province’s policy shift to the Ontario Health Team model has provided a substantial opportunity for East Toronto to spread and scale the work we have already started, as well as creating new platforms for change and innovation across all our provider partners. In our application we have identified specific actions the provincial government can take to help us accelerate our efforts (including addressing policy barriers, providing resources and funding support in specific areas, and supporting provincial digital solutions), which we would be pleased to discuss further. We are excited to submit our full application and are confident that we are ready to be one of the province’s first Ontario Health Teams.
Sincerely,
Anne Babcock
President and CEO, WoodGreen Community Services
On behalf of the East Toronto Health Partners
Copy/
Dr. Rueben Devlin, Special Advisor and Chair of the Premier’s Council on Improving Healthcare and Ending Hallway Medicine
Helen Angus, Deputy Minister, Ministry of Health
Marie-Lison Fougère, Deputy Minister, Long-Term Care
East Toronto Health Partners